Calag Archive
Calag Archive
Online training for child care providers teaches child nutrition in English and Spanish
Publication Information
California Agriculture 76(4):131-140. https://doi.org/10.3733/ca.2022a0015
Published online February 09, 2023
PDF | Citation | Permissions
NALT Keywords
Abstract
Poor nutrition among young children is a national health crisis which contributes to obesity and chronic disease later in life. Since children spend so much time in child care, child care providers can help improve the quality of young children's nutrition and foster lifelong healthy eating habits. However, California's family child care home (FCCH) providers receive little training on what and how to feed young children. To address this problem, we developed a self-paced online training on child nutrition in English and Spanish for FCCH providers. Our feasibility study evaluated providers’ satisfaction with the training and ease of use, using an online survey and a 45-minute interview upon completing the training. Providers rated their training experience as excellent, easy to enroll in, and complete. Most providers reported they were somewhat likely to make changes to what and how they feed infants and toddlers. Many recommended adding printed resources and culturally relevant material for future trainings.
Full text
Childhood obesity is a major public health crisis in the United States (Skinner et al. 2018). Thirty percent of children do not consume any vegetables on a daily basis, with up to 15% of their calories coming from foods and beverages with added sugars (Butte et al. 2010; Fox et al. 2010; Weinfield et al. 2019). These unhealthy childhood eating habits contribute to adult health problems such as diabetes and heart disease (Reilly et al. 2011).
Child care is an ideal environment in which to improve young children's eating habits. Over half of young children spend an average of 30 hours per week in child care, where many of them consume the majority of their daily calories (Benjamin-Neelon 2018; Laughlin 2013; Leucking et al. 2020). Because of this, providers serve as influential adults who can shape lifelong healthy eating habits and reinforce them as part of children's daily routines (Deiner and Qiu 2007).

Findings from a UC Cooperative Extension study suggest that online trainings are an effective way for public health educators to convey important nutritional information to family child care home providers. Photo: Danielle L. Lee.

Family child care home providers serve as influential adults who can shape lifelong healthy eating habits and reinforce them as part of children's daily routines. Photo: Danielle L. Lee.
Family child care homes (FCCH) are a type of licensed child care provided in private homes. Approximately one in five children in the U.S. will attend an FCCH at some point before entering kindergarten (National Association of Child Care Resource and Referral Agencies 2010). FCCHs are typically located in the same neighborhood as the families they serve. They provide longer hours of care and are lower in cost than child care centers. FCCH providers in the U.S. are ethnically diverse and often appeal to underserved families with limited income who may face challenges with healthy eating habits due to systemic social inequities (Min et al. 2018; Whitebook et al. 2006). Evidence suggests that children cared for in FCCHs may be at greater risk of obesity than those cared for in their own home or in child care centers (Ward et al. 2017).
California has over three times the number of licensed FCCHs (about 30,000) as child care centers (Child Care Aware of America 2020). Compared to staff working in centers, FCCH providers experience numerous barriers to providing children with healthy meals and snacks. This is a missed opportunity for FCCH providers to support children's healthy eating habits.
Few nutrition standards apply to licensed FCCHs that are not participating in the federal Child and Adult Care Food Program (CACFP) (Lee et al. 2020). One specific regulatory gap is the California Health and Safety Code, which requires licensed centers but not licensed FCCH providers to adhere to CACFP nutrition standards regardless of program participation (Lee et al. 2020). An attempt to extend this requirement to FCCH providers in 2012 through the Improving Child Care Nutrition Act (CA AB 1872) passed both the California Assembly and Senate but was vetoed by the governor (California Legislative Information 2021). Attempts to mitigate this gap were implemented in 2016 with a California law that requires newly licensed FCCH providers to complete one hour of nutrition training (California Emergency Medical Services Authority 2021). However, this leaves out nearly 30,000 FCCH providers in California licensed prior to 2016 who provide care to over 310,000 children (California Department of Social Services, unpublished data). In general, few nutrition interventions have been conducted in FCCHs (Benjamin-Neelon et al. 2018; Ward et al. 2017).
To address the training needs of FCCH providers, a multi-disciplinary, bilingual team of nutrition and health experts developed an in-person workshop in English and Spanish to share best practices on what and how to feed young children (Ritchie et al. 2020, 2021). Given that one in 10 FCCH providers in California prefer to speak only Spanish and about one-quarter prefer Spanish in addition to English, a Spanish-language training was essential (Whitebook et al. 2006). The team conducted a three-month pilot study of the workshop and found that, although the FCCH providers adopted many of the recommended feeding practices (Box 1), attending the workshop was challenging due to providers’ busy schedules and transportation needs (Ritchie et al. 2020, 2021). To improve accessibility and sustainability, the workshop content was converted to an interactive, online training with a digital teacher avatar named “Laura,” which included videos, games and quizzes. The purpose of this feasibility study was to evaluate FCCH provider satisfaction with and ability to complete the self-paced English and Spanish online training.
Box 1
Recommended practices on what and how to feed young children adopted by family child care home providers after completing a two-hour in-person workshop
Infant feeding recommendations:
-
Supporting and encouraging breastfeeding
-
Providing adequate refrigeration for storing breastmilk
-
Introducing solid foods gradually and waiting 3–5 days before introducing new foods
Toddler feeding recommendations:
-
Offering natural cheese no more than 1–2 times per day
-
Using only liquid non-tropical vegetable oils
-
Providing meals and snacks every 2–3 hours at regularly scheduled times
-
Minimizing distractions while eating
-
Offering healthy items at celebrations
-
Rarely or never offering 100% fruit juice
-
Not serving white grains
-
Not serving high-salt foods
-
Not serving cheese food or cheese spread
Interactive online training
The online training was modified into an audio-narrated, interactive training from materials previously developed for the in-person workshop. Content was reviewed by the research team, which included University of California Cooperative Extension (CE) specialists and nutrition, family and consumer sciences advisors.
The in-person training pilot test (Box 2) showed that providers were seldom following certain key recommended practices. These practices were singled out for additional reinforcement via videos, interactive games, and quizzes. The videos were recorded during meals at two FCCH sites, while a registered dietitian developed the quizzes and games. The final content included four 20-minute modules on what and how to feed infants (0–11 months; two modules) and toddlers (12–36 months; two modules) (figs. 1 and 2).
Box 2
Recommended practices on what and how to feed young children with low or no adherence by family child care home providers after completing a two-hour in-person workshop
Infant feeding recommendations:
-
Offering only breastmilk and/or infant formula as beverages (besides water)
-
Encouraging older infants to self-feed with their fingers and drink from a cup with assistance
-
Feeding younger infants on demand
-
Holding infants while bottle-feeding
-
Not propping bottles or allowing infants to carry or sleep with bottles
-
Including older infants at family-style meals where the provider and children eat together
Toddler feeding recommendations:
-
Ensuring water is easily available for self-serve and is actively offered with meals and snacks
-
Serving meals family-style and teaching children to serve themselves
-
Expecting children to eat a lot at some meals and little at others, to not eat everything offered, change likes and dislikes, be messy, and take time to accept new foods
-
Not pressuring children to eat or clean their plates
-
Not focusing mealtime conversations on the amount eaten
Materials were translated into Spanish by a bilingual CE translator and converted into online modules. The resulting Spanish materials were reviewed and revised as needed by a CE specialist with expertise in linguistically appropriate nutrition education materials for Spanish-speaking populations. Under guidance from the CE specialist, several of the recommended food items were included in the training to ensure cultural inclusivity (e.g., traditionally made whole-grain corn tortillas). Adobe Articulate 360 software was used to create the four interactive modules. Each module was designed to be completed in about 20 minutes. Audio content was narrated in Spanish and English.
Topics covered in the online training were what and how to feed infants and toddlers. What to feed infants and toddlers included recommendations for milk beverages (toddlers only), grains, proteins, other dairy products, fruits, vegetables, sugar and salt. How to feed infants and toddlers included recommendations for breastfeeding and bottle feeding (infants only), introducing solid foods (infants only), preventing choking, meal and snack frequency (toddlers only), culturally relevant foods, healthy food at celebrations, the feeding environment, and responsive feeding (which are feeding practices that encourage the child to eat autonomously and in response to physiological and developmental needs (Pérez-Escamilla et al. 2021)).
The training also offered information on what not to feed infants and toddlers: juice, soda, sugar-free drinks, juice drinks, coffee, sweet tea, sports drinks, lemonade or aguas frescas, horchata, energy drinks, cow's milk (infants only) and plant-based milks (infants only); white or enriched bread, white rice, flour tortillas, pasta or noodles made from white flour; desserts such as cake, cookies, pie, pastries or donuts; processed meats or deep fried or pre-fried meats, poultry and fish; cheese spreads, imitation cheeses, unpasteurized or raw dairy products; deep fried or pre-fried baked vegetables; canned fruits and vegetables with added salt, sugar or fat; foods with added sugar/sugar equivalents, food with a combination of three or more kinds of sugar/sugar equivalents, low-calorie sweeteners, and honey (infants only); high salt foods (>200 mg sodium for snacks, >480 mg sodium for entrees), or adding salt to food for infants.
The training was made available in an online training portal to facilitate public access (Lee et al. 2022a, 2022b, 2022c, 2022d). Final training modules were exported as Sharable Content Object Reference Model (SCORM) files and uploaded to eXtension Campus, which provides online research-based curricula. Upon logging into the eXtension Campus online portal and enrolling in the online trainings, participants received a welcome message describing what to complete — “Part 1: What to Feed” module and “Part 2: How to Feed” module — to receive a certificate of completion. When participants clicked on the training module links, they were redirected to a new browser window where the interactive training appeared with a digital teacher avatar named “Laura” to guide them through the content of each module (fig. 1).
FIG. 1. An interactive menu in the online training. A virtual online training instructor guides students through an interactive menu of sections of the online training that students are required to complete.

FIG. 2. An interactive game in the online training. Student knowledge is tested throughout the training using interactive quizzes and games similar to this one.
Evaluating the training
FCCH providers (n = 10; half English- and half Spanish-preferring) were recruited using convenience sampling through California CE networks. Recruitment emails and fliers were distributed by local child care resource and referral networks. In the recruitment email, providers were asked to complete a brief online survey to determine whether they were eligible to participate. Eligible providers had to have been in operation for more than one year, care for at least one infant and one toddler age 1–2 years old, provide at least one meal, one snack, and one beverage daily, be able to speak and read English or Spanish, and have access to a computer, laptop, smart phone, or tablet with internet connection. Participation required three hours of each provider's time. Each participant was compensated with a $50 gift card. The University of California, Davis, Committee for the Protection of Human Subjects deemed the study exempt.
Enrolled providers received email instructions to create an account on eXtension Campus and to enroll in the online trainings. After completing the four 20-minute modules, providers were emailed a link to a brief Qualtrics online survey and were scheduled to complete a 45-minute interview via Zoom or by telephone with a bilingual Nutrition Policy Institute researcher.
The main evaluation outcomes measured were: providers’ ratings of the online training, what information was helpful or new to them, and if the training promoted changes to what and how they feed infants and toddlers in their care. We also aimed to understand the unique experiences of providers who took the Spanish version of the online training.
Research team members developed survey questions to evaluate the online training. Providers were asked to rate the training registration, format, clarity, amount and usefulness of information, quality, length, ease of completion, and overall experience. They were also asked about the likelihood of making changes to what and how they would feed infants and toddlers based on what they learned in the training. Finally, providers were asked if they would recommend the training to other providers and if it would be helpful to have a nutrition educator available to discuss what they learned. The survey (available in the online technical appendix) captured provider demographics, characteristics of the FCCH and the children they cared for, where they received information on nutrition related to their work, and how they shared information with parents.
Research team members developed structured interview questions (available in the technical appendix) to explore providers’ experiences with registering for and completing the training. Questions were repeated for each of the four modules to determine what information was new, helpful, not helpful, repetitive, or confusing. Spanish-preferring providers were asked about their country of origin, length of time living in the United States, and questions about the clarity of wording and phrases, ease of following the narrative, training recommendations that they perceived to be relevant or problematic for Spanish-preferring providers and families, and perceptions of Spanish-preferring providers’ comfort with an online training.
English and Spanish interviews were recorded and transcribed. English Zoom recordings were transcribed using Zoom's built-in transcription feature. Spanish Zoom recordings were transcribed by a researcher fluent in both Spanish and English. Researchers then reviewed and revised the English Zoom transcriptions and Spanish researcher transcriptions while simultaneously reviewing the audio recordings. Spanish transcriptions were translated into English for analysis.
Survey data were analyzed in Excel (Microsoft Office 2019) using descriptive statistics. Interview data were analyzed using an inductive approach for qualitative evaluation data (Thomas 2006). Interview responses were tabulated by interview question for each participant, then reviewed by two investigators, and coded for themes. One researcher conducted the initial review and developed the original coding scheme; the second researcher conducted the second review using codes developed by the initial reviewer. Disagreements in coding were discussed to reach consensus on final coding. Themes were summarized for each module and key quotes for each theme were extracted.
Providers’ training satisfaction
Providers were all women, with an average age of 54. A majority identified as Hispanic and had some college or an associate's degree. Providers cared for an average of nine children, nearly half of whom qualified for child care subsidies (table 1). All providers participated in CACFP; most reported receiving information about nutrition related to their work as child care providers from CACFP, from the families of the children they cared for, and from friends. Providers reported sharing nutrition information with the parents or caregivers primarily via printed handouts or flyers, bulletin boards, text messages, or in-person meetings. The Spanish-preferring providers interviewed were from Nicaragua or Mexico and had lived in the United States for 30–35 years.
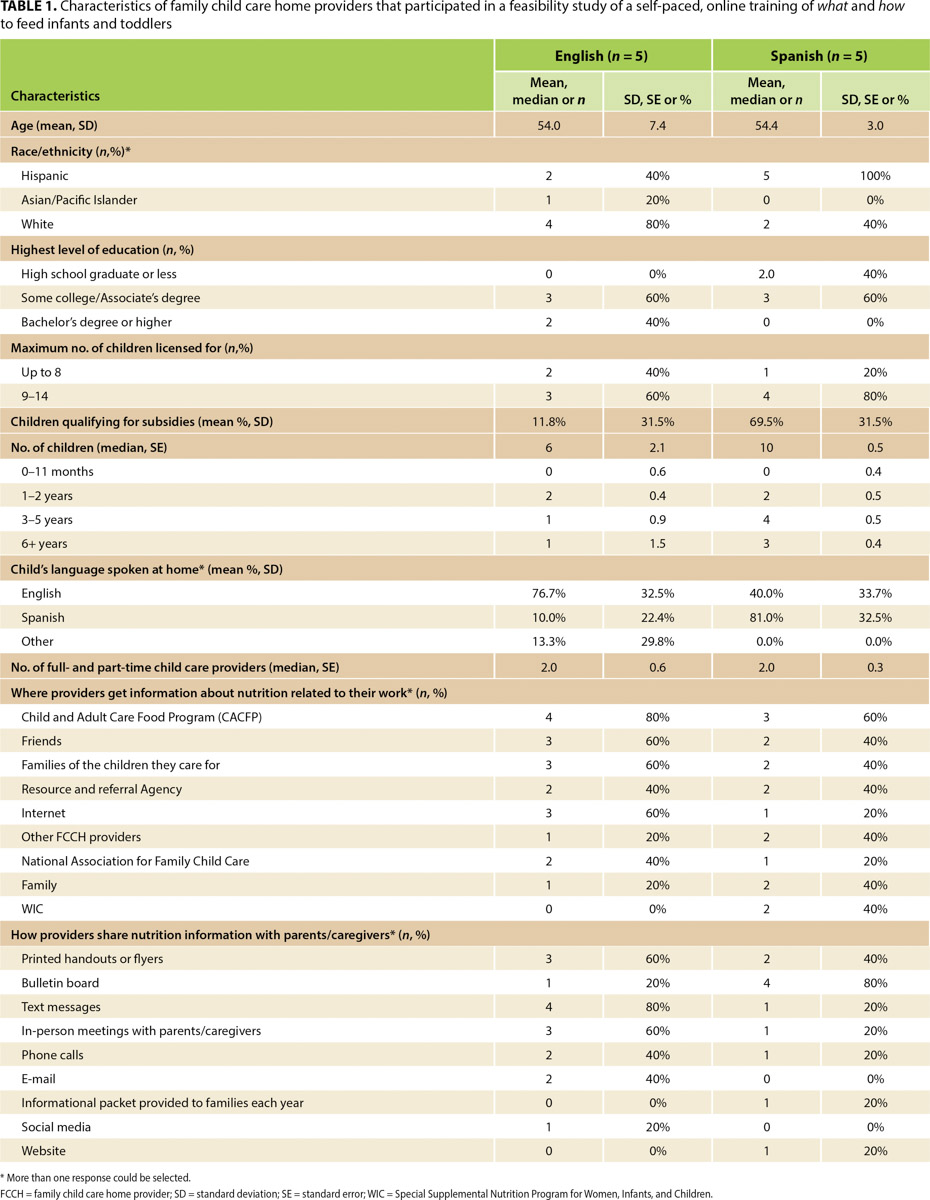
TABLE 1. Characteristics of family child care home providers that participated in a feasibility study of a self-paced, online training of what and how to feed infants and toddlers
The English and Spanish versions of the online training were rated favorably by FCCH providers (table 2). Providers (n = 10) rated the registration for the online training (Mean[SD] 4.4[0.84]), training format (4.2[0.79]), clarity (4.8[0.63]) and amount (4.6[0.52]) of the information, usefulness (4.5[0.85]), quality (4.6[0.52]), length (4.7[0.48]), and overall experience (4.8[0.42]) of the training as good (based on a 5-point scale of 1 = very poor to 5 = excellent). Providers were somewhat likely to make changes to what (4.3[1.34]) and how (4.3[1.34]) they feed infants and toddlers in their care after completing the training and were very likely (4.8[0.63]) to recommend the online training to other providers (based on a 5-point scale of 1 = very unlikely to 5 = very likely). They found the training easy to complete (4.2[1.14], based on a 5-point scale of 1 = very hard to 5 = very easy). Seventy percent of providers thought it would be helpful to have a nutrition educator available to discuss what they learned after taking the online training.

TABLE 2. Family child care home providers’ evaluation of a self-paced online training on what and how to feed infants and toddlers
Providers indicated in interviews that the English and Spanish versions of the online trainings were well received, that they learned new and helpful information from each of the four modules, and that there was little to no information that was too repetitive or unhelpful. Only one provider, who reported low technical literacy, had difficulty in completing the online course registration and navigating the online training.
Key themes of what information was new and helpful are summarized in table 3. Generally, providers had more to say about the novelty and usefulness of the training content on how to feed infants and toddlers compared to what to feed them. Many providers said the training was both a good refresher for more experienced FCCH providers and a good resource for new FCCH providers:
Right now we are not in many classes and this refreshes us.
It would help the people who are starting their business. It's very well explained.
I recommend it for new providers who don't maybe know what to feed the kids. I think it's a very good introduction. For me, it was a lot of repeat, but it's good because I don't always have infants all the time…. So it was a good refresher.
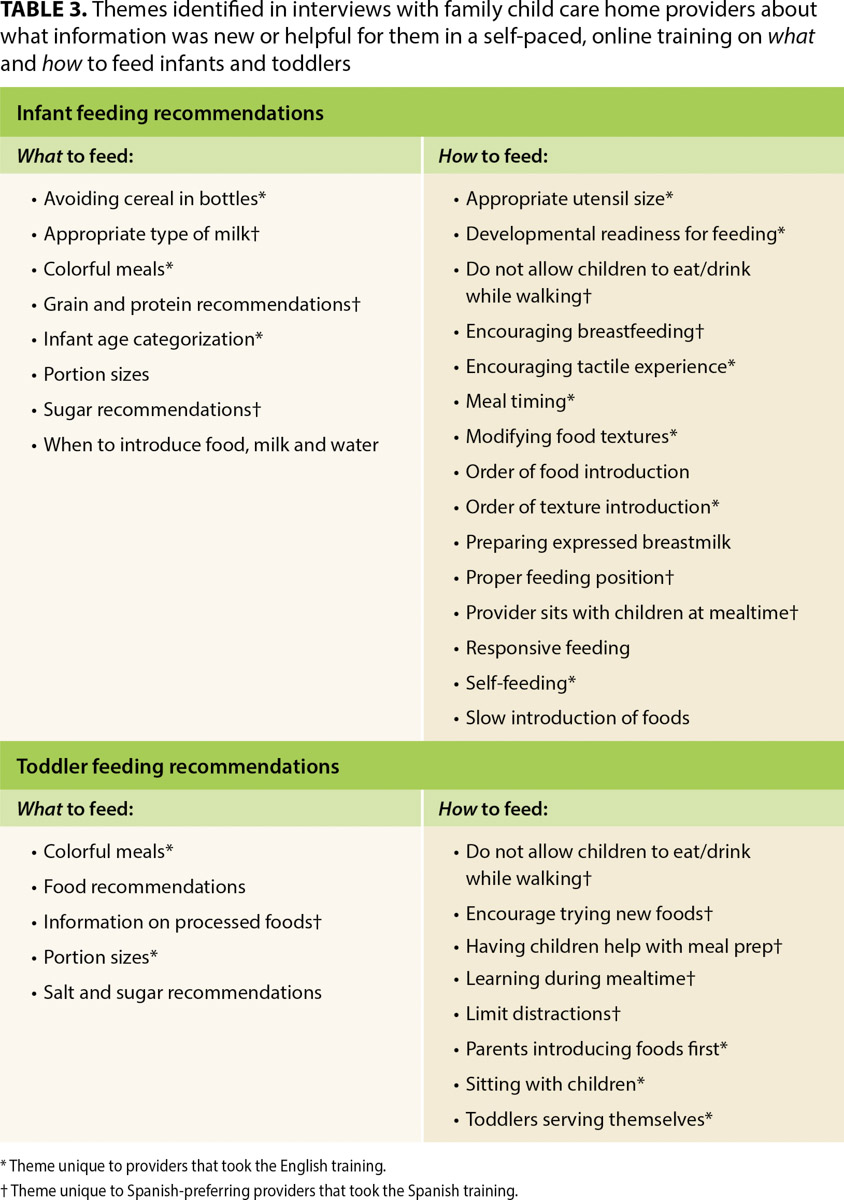
TABLE 3. Themes identified in interviews with family child care home providers about what information was new or helpful for them in a self-paced, online training on what and how to feed infants and toddlers
Interaction is important
Providers expressed appreciation for the interactive aspects of the training, such as quizzes, and recommended including more interactive features in future versions. Additional suggestions included introducing more advanced modules for more experienced FCCH providers and facilitating access for providers with limited technical proficiency. One provider said,
You know that's the hardest part about doing this for so long it's finding seminars and classes that aren't really geared for newer providers.
Providers suggested providing a digital one-page summary of key recommendations to print and post in their home and to share with parents. They noted that their efforts to convey information on child feeding practices to parents are often met with mistrust or skepticism, so they felt that a summary from a trusted source such as the University of California would provide them with much-needed credibility. This indicates that providing support and resources may positively impact parent engagement outcomes and bolster the confidence of FCCH providers to sustain these practices. One provider said,
… giving [parents] a little referral or a little article or fact sheet from somebody that has a name on it seems to make more impact on them. Summaries, that would have been nice to be able to print that out and then to hand it to my parents.
Cultural relevance
An additional theme identified during provider interviews was the need for improved cultural relevance and sensitivity of the content of the online trainings. On the topic of food recommendations, one provider said,
… as I mentioned we are vegetarian, so of course the meat section is definitely not something that I wanted to know about. But the person who eats meat, it's helpful for them. I mean it might be done in such a way that if you don't eat meat at all, you might give an option to skip that section.
Providers recommended efforts to tailor the Spanish-language version for providers from different regions of Latin America. A Spanish-preferring provider said,
We Americans — Central Americans, North Americans, South Americans — are used to giving cow's milk, it's the most common, but [people in] some other places also consume goat's milk. But I know that in other cultures they do not consume cow's milk or goat's milk, only vegetable milk.
On the topic of utensils, one provider said,
Here it says use dishware and utensils that are sized appropriately… I mean in India we practice using hands to eat, right. So are you recommending that we should give utensils to infants for them to learn to eat?
On the topic of portion sizes, a Spanish-preferring provider said,
It seems to me that perhaps we should talk about the portions. It can be cultural. The customs of each country, of each person, affects us a lot.
Spanish-preferring providers
Themes unique to Spanish-preferring providers’ experience of the online training emerged. Data in tables 1 to 3 are presented by training language to highlight experiential differences from those who took the training in English. In general, more Spanish-preferring providers (40% vs. 0%) reported using the federal Special Supplemental Nutrition Program for Women, Infants and Children (WIC) for nutrition information related to their job (table 1). More Spanish-preferring providers reported sharing nutrition information with parents and caregivers using bulletin boards (80% vs. 20%) compared to more technology-based methods (e.g., text messages, phone calls, emails) (table 1). More Spanish-preferring providers (60% vs. 0%) reported it would be helpful to have a nutrition educator available to discuss the online trainings (table 2).
Regarding new or useful information, several unique themes were found from interview responses from Spanish-preferring providers in the training (table 3). Specifically for infant feeding recommendations, Spanish-preferring providers reported the following as new or useful: appropriate milk type; grain, protein, and sugar recommendations; not allowing children to eat or drink while walking; encouraging breastfeeding; proper feeding positions; and sitting with children during mealtimes. Specifically for the toddler feeding recommendations, Spanish-preferring providers reported the following as new or useful: information on processed foods; not allowing children to eat/drink while walking; having children help with meal prep; facilitating learning during mealtime; and limiting distractions during mealtime.
Providers also reported that the Spanish version of the online training was clear, the narrative was easy to follow, and the information and recommendations provided would be particularly relevant for Spanish-preferring providers. One provider said,
I think that if it's very well explained and yes they [Spanish-preferring providers] would understand it and it would help the people who are starting their business.
Spanish-preferring providers highlighted only a few recommendations in the training that might not appeal to other providers. One was the recommendation on whole grains and whole foods, with two providers citing cost as a barrier, in addition to cultural preference.
Like whole grains, like brown rice. … It's that there are people who prefer to consume white rice because it's what they like… so there is the cultural preference of each one …
I know of many Hispanic providers who don't do it because they don't like it. It is not the type of food that they are used to, so there's cultural controversy and also monetary. [They say,] “Don't use that. It's more expensive. The price is higher to consume brown rice than the rice that we can consume as a family of moderate resources.”
Some people may not be economically facilitated to have that level and buy that type of food. I'm talking like organic food or whole food. Like whole grains, like brown rice.
Two providers reported hearing unfamiliar terms in the online training. A provider from Nicaragua noted a lack of familiarity with the Spanish term used for lean meat, while a provider from Mexico reported unfamiliarity with some terms used for fruits. A glossary of terms used in different Spanish-speaking regions may be a useful addition for the online training.
Online training fills a need
FCCH providers reported high levels of satisfaction with the 80-minute online training in both English and Spanish, with most saying they intended to make changes to what and how they feed infants and toddlers. They said the training taught them new information and also reminded them of old information they had forgotten. These findings and other studies suggest that not only are online trainings a good fit for this population, but are in fact preferred by child care professionals (Ackerman 2017; Cotwright et al. 2020; Lee et al. 2021; Rheingold et al. 2012; Weigel et al. 2012). One study showed that an online training on healthy beverages makes it more likely that FCCH providers will follow these recommendations (Lee et al. 2021).
These online trainings are especially important because they may help fill the gap in California law which does not hold FCCHs to the same nutritional standards as other daycare providers. This online training is publicly available on the eXtension Campus (Lee et al. 2022a, 2022b, 2022c, 2022d) to any FCCH provider who has access to a computer, smart phone, or tablet with internet connection. FCCH providers in California can take the training for free; FCCH providers in other states pay $15.
Despite our attempts to ensure that the online training was culturally sensitive, Spanish-preferring providers suggested making the training more inclusive and culturally relevant to their specific demographic. (Given the brevity of the online training, it is difficult to be inclusive of all cultures.) FCCHs homed in on certain food (specifically whole grains) and beverage items, utensils, and the need to take into account those providers who maintain vegetarian-only FCCHs. Other studies have also suggested similar cultural perceptions around white rice and the unfamiliarity with brown rice and other whole grains in non-white populations (Monge-Rojas et al. 2014). Studies comparing Latinx vs. non-Latinx FCCH providers have found similar differences in nutrition-related attitudes, specifically around what and how to feed young children (Jiang et al. 2021). Several studies highlight the effectiveness of culturally tailored nutrition guidelines for young children in child care who come from ethnically diverse, low-income families (Gans et al. 2009; Hammons et al. 2019; Kaiser et al. 2015; Looby et al. 2020; Smith et al. 2004). Additionally, over half of Spanish-preferring providers in this study said it would be helpful to have a nutrition educator available to talk to after the online trainings.
One of the big challenges to implementing food recommendations, the providers reported, is higher costs. Studies have shown that the higher cost for more nutritious food is an obstacle for FCCHs (Dev et al. 2020; Earnesty et al. 2022; Lee et al. 2018; Monsivais et al. 2012). (Despite the small financial incentive provided to FCCH providers to participate in our evaluation, we made no attempts to offset the cost of implementing the recommendations.) However, programs such as CACFP have been effective in providing financial support to help FCCHs improve their food and beverage offerings (Gurzo et al. 2020; Lee et al. 2018; Monsivais et al. 2011). Pairing online training with financial assistance for FCCH providers to implement the recommendations proposed in the online training should be explored.

The online child nutrition trainings are especially important because they may help fill the gap in California law, which does not hold FCCHs to the same nutritional standards as other daycare providers. Photo: Danielle L. Lee.
This study has both strengths and limitations. A key strength of the study is the mixed methods approach of gathering both qualitative and quantitative data. Another strength is the online format of the training, which is a convenient option — and possibly the only option — for busy FCCH providers, especially during the COVID-19 pandemic. The principal limitation was the small sample size, the convenience sampling, and the limited representation of non-white or non-Hispanic providers. As a result, these findings may not be representative of all FCCH programs across California or the United States.
The benefits of the self-paced online trainings are that they are easily accessible and provide a conducive environment for supportive learning and reinforcing helpful information. Our findings suggest that these online trainings are an especially effective way for public health educators to convey important nutritional information to FCCHs across a diverse set of ethnic and language groups. Moving forward, future research should evaluate the efficacy of pairing the online training with financial support to encourage FCCH providers to adopt better nutriton practices in order to improve children's health outcomes.
Online training for child care providers teaches child nutrition in English and Spanish

